CAM-C : improving screening for hepatitis C in Cambodia
Last updated on 21 October 2025
Cam-C: the benefits of community-based approaches
- In Cambodia, Hepatitis C virus (HCV) is a public health challenge, especially among adults over 40.
- The CAM-C study compared community-based and facility-based strategies to improve HCV testing uptake. Results showed that the community-based approach, involving Community Health Workers to conduct rapid tests, was more effective.
- Further analysis will be conducted in order to investigate cost-effectiveness.
In brief
Investigator / Co-investigator
Pr. Vonthanak SAPHONN, University of Health Sciences, Cambodia
Pr. Jean-Charles DUCLOS VALLEE, Hepatobiliary Centre – Paul Brousse Hospital, France
Pathology
Hepatitis C
Teams
University of Health Sciences, Phnom Penh, Cambodia, Hôpital Paul Brousse, Villejuif, France, Fond. Merieux, Cambodia, Inserm SC10/US019, Villejuif, France, UMR1252 SESSTIM/ORS PACA, Marseille, France
Status
Completed
CAM-C study methodology
Context
In Cambodia Hepatitis C virus (HCV) is a major public health concern with an estimated prevalence around 5%among adults aged more than 45 years (compared to only 0.6% among younger). Improving screening and treatment is crucial, although new strategies are needed. Community-based approaches could be a facilitator to reach people, especially those far away from healthcare facilities. This study contributes to the broader national effort to eliminate hepatitis C by 2030.
Objective of the study CAM-C
The objective of this study is to compare the effectiveness of a community-based strategy to a facility-based strategy in improving the uptake of HCV antibody rapid testing (HCV-RDT) and increasing awareness of the results among Cambodians aged over 40 years.
Methods
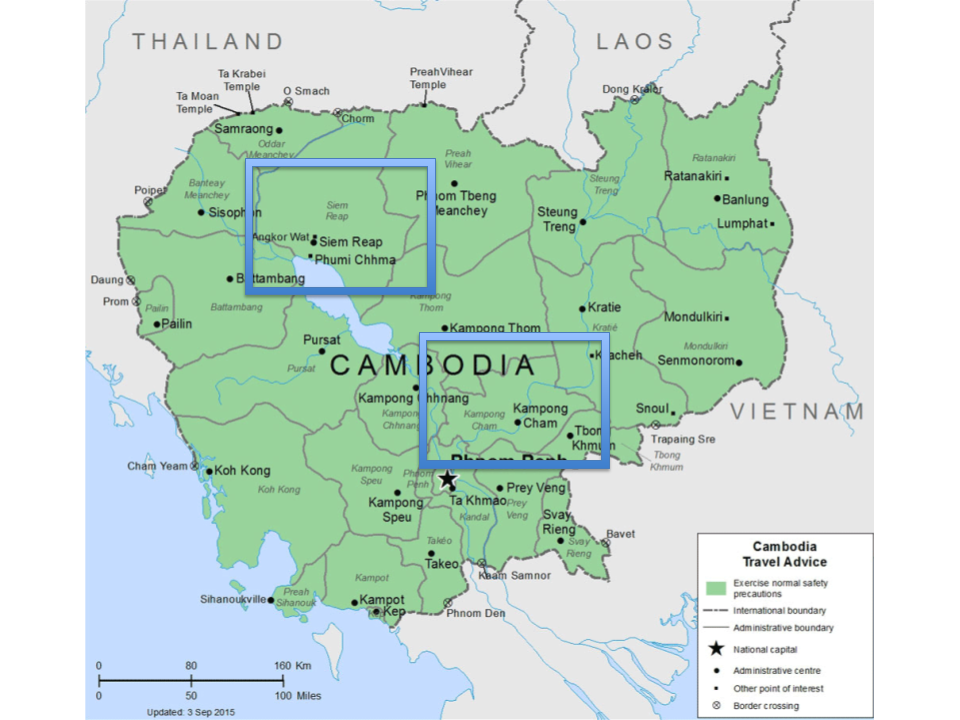
ANRS 12384 Cam-C was a two-arm cluster-randomized controlled trial. It was conducted in the Kampong Cham and Siem Reap Provinces. A total of 8 geographical areas were selected: 4 in each province to be part of arm 1 (facility-based) and arm 2 (community-based). A cluster was defined as a group of 50 households resulting in 160 clusters: i.e., 80 per province, 20 per geographical area.
- Arm 1: Facility-based testing intervention
Community Health Workers (CHWs) provided information on the possibility to be tested in health centers for HCV infection. If the participant agrees to participate, she/he will receive a voucher to go to a referral health center where HCV RDT was conducted, and if positive, blood samples were collected for HCV RNA tests.
- Arm 2: Community-based testing intervention
After a dedicated training, CHWs will do the HCV RDT on a finger stick capillary whole blood directly in the participant’s household. In case of structural or societal barriers for household testing, it will be possible to provide testing in a specific location in the village. Blood spots were collected immediately on DBS (dried blood spot) for HCV RNA tests if HCV RDT positive.
Study area Siem Reap and Kampong Cham provinces.
The study showed community-based approach to be effective as it improves the uptake of HCV antibody rapid testing compared with the facility-based approach.
Results of the CAM-C study
The first results were presented at the AIDS 2024 conference. A total of 7692 participants, 3861 facility-based and 3831 community-based, were enrolled between April and July 2022. The median [IQR] age was 55 [47-65] years.
After adjusting for covariates and controlling for the cluster design, community-based group had higher odds of HCV RDT testing uptake compared to facility-based group (OR=2.18, IC 95% :1.28-2.04).
The study showed community-based approach to be effective as it improves the uptake of HCV antibody rapid testing compared with the facility-based approach. These results demonstrate that training and involving Community Health Workers in HCV screening should be considered for the scale-up of the community-based strategy. However, more attention should be given to males and single people as they seem to be relatively less reached by the Community Health Workers activities (e.g. maybe more absent from households at the time of the activities). This suggests that CHWs’ HCV screening activities should be extended to places where males and single people could be reached, for example, in workplaces or other meeting points of single people. Further analysis will be conducted to investigate whether the community-based strategy is cost-effective.
Scientific publications
- Khuon D, Sagaon-Teyssiera L, Netha S, et al. Community-based versus facility-based services to improve hepatitis C screening in Cambodia: a cluster randomized controlled trial (ANRS 12384 Cam-C study). The Lancet Regional Health – Western Pacific. 2025 oct;63, 101703.
- Mosnier E, Ségéral O, Neth S, et al. Community Versus Facility-Based Services to Improve the Screening of Active Hepatitis C Virus Infection in Cambodia: The ANRS 12384 CAM-C Cluster Randomized Controlled Trial-Protocol for a Mixed Methods Study. JMIR Res Protoc. 2024 Nov 20;13:e63376. doi: 10.2196/63376.
Our selection

ANRS HEPDELTA cohort
National cohort of patients co-infected with hepatitis B and Delta viruses
24 July 2024

ANRS PRINCESSE cohort
PrEP, sexually transmitted infections, contraception, viral hepatitis B, sexual health for sex workers in Côte d’Ivoire
22 July 2024